Reoperation in Horizontal Strabismus and its Related Risk Factors
Medical hypothesis discovery and innovation in ophthalmology,
Vol. 7 No. 2 (2018),
1 June 2018
,
Page 73-82
Abstract
This study was performed to determine the surgical outcomes and the related risk factors of second operation in patients with residual horizontal deviations. In this interventional case series study, a total of 119 patients with a history of reoperation were included (39 exotropia and 80 esotropia). Cases with consecutive strabismus, muscular palsy, systemic disease, lack of ocular fixation, and those, who had vertical deviation and Dissociated Vertical Deviation (DVD)>5 Prism Diopters (pd) were excluded. Medial Rectus (MR) resection in residual Exotropia (XT) and Lateral Rectus (LR) resection in residual Esotropia (ET) were performed. Unilateral or bilateral operations were considered if the preoperative residual deviation was < 20 pd or > 20 pd, respectively. Success of the reoperation was considered if the postoperative angle of deviation was ≤ 10 pd. Unilateral and bilateral MR resection was performed in 26% and 74% of patients with XT, respectively, with greater dose response in unilateral cases (2.8 versus 2.6 mm/pd). Successful surgical outcomes were observed in 94.9% of patients with XT. Unilateral and bilateral LR resection was also performed in patients with residual ET, each in 50% of patients. Unilateral cases showed greater dose-response compared to bilateral ones (2.6 versus 2 mm/pd) and successful surgical outcomes were observed in 83.8% of patients with ET. No variable was found as a risk factor of reoperation in both groups. In conclusion, both LR and MR resection are easy and predictable surgical approaches with high success rate in patients with residual ET and XT. Generally, MR resection is more effective than LR resection. Unilateral operation is less recommended in the residual exotropic group, due to its lower success compared to the bilateral operation. Unfortunately, none of the mentioned variables were found to be the risk factor of reoperation in the sampled patients.Â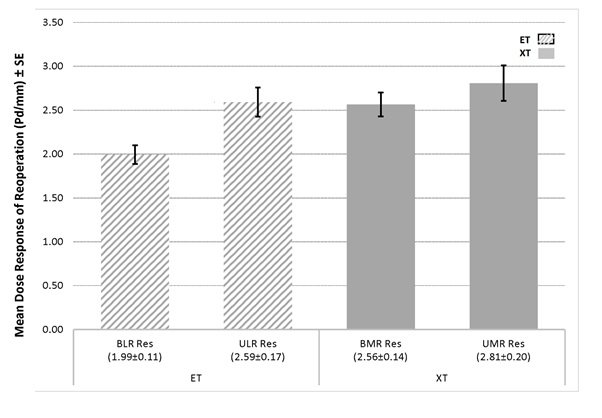
References
Lee S, Lee YC. Relationship between motor alignment at postoperative day 1 and at year 1 after symmetric and asymmetric surgery in intermittent exotropia. Jpn J Ophthalmol. 2001;45(2):167-71. pmid: 11313049
Lee JY, Choi DG. The clinical analysis of recurrence after surgical correction of intermittent exotropia. J Kor Ophthalmol Soc. 2002;43(11):2220-6.
Lim SH, Hong JS, Kim MM. Prognostic factors for recurrence with unilateral recess-resect procedure in patients with intermittent exotropia. Eye (Lond). 2011;25(4):449-54. doi: 10.1038/eye.2011.12 pmid: 21311571
Hahm IR, Yoon SW, Baek SH, Kong SM. The clinical course of recurrent exotropia after reoperation for exodeviation. Korean J Ophthalmol. 2005;19(2):140-4. doi: 10.3341/kjo.2005.19.2.140 pmid: 15988932
Wang T, Wang L-H. Surgical treatment for residual or recurrent strabismus. Int J Ophthalmol. 2014;7(6):1056.
Mewis L, Tang RA, Mazow ML. See-saw nystagmus after strabismus surgery. J Pediatr Ophthalmol Strabismus. 1982;19(6):302-5. pmid: 7153822
Rajavi Z, Ghadim HM, Ramezani A, Azemati M, Daneshvar F. Lateral rectus resection versus medial rectus re-recession for residual esotropia: early results of a randomized clinical trial. Clin Exp Ophthalmol. 2007;35(6):520-6. doi: 10.1111/j.1442-9071.2007. 01548.x pmid: 17760633
Yazdian Z, Ghiassi G. Re-recession of the lateral rectus muscles in patients with recurrent exotropia. J AAPOS. 2006;10(2):164-7. doi: 10.1016/j.jaapos.2005.11.014 pmid: 16678753
Velez FG, Thacker N, Britt MT, Alcorn D, Foster RS, Rosenbaum AL. Rectus muscle orbital wall fixation: a reversible profound weakening procedure. J AAPOS. 2004;8(5):473-80. doi: 10.1016/S1091853104001314 pmid: 15492742
Saxena R, Phuljhele S, Sharma P, Pinto CN. Periosteal Fixation Procedures in the Management of Incomitant Strabismus. Middle East Afr J Ophthalmol. 2015;22(3):320-6. doi: 10.4103/0974-9233.159736 pmid: 26180470
Buck D, Clarke MP, Haggerty H, Hrisos S, Powell C, Sloper J, et al. Grading the severity of intermittent distance exotropia: the revised Newcastle Control Score. Br J Ophthalmol. 2008;92(4):577. doi: 10.1136/bjo.2007.120287 pmid: 18369078
See A. A and V patterns of fixation, 319-320 etiology of, 77-78 indications for surgical correction, 74 normosensorial cases of, 73. Age. 2015;227:228.
Ortiz S, Borchert M. Long-term outcomes of pediatric ocular myasthenia gravis. Ophthalmology. 2008;115(7):1245-8 e1. doi: 10.1016/j.ophtha.2007.10.022 pmid: 18155768
Kupersmith MJ. Ocular myasthenia gravis: treatment successes and failures in patients with long-term follow-up. J Neurol. 2009;256(8):1314-20. doi: 10.1007/s00415-009-5120-8 pmid: 19377863
Yang HK, Hwang JM. Bilateral vs unilateral medial rectus resection for recurrent exotropia after bilateral lateral rectus recession. Am J Ophthalmol. 2009;148(3):459-65. doi: 10.1016/j.ajo.2009.04.017 pmid: 19541284
Gunasekera LS, Simon JW, Zobal-Ratner J, Lininger LL. Bilateral lateral rectus resection for residual esotropia. J AAPOS. 2002;6(1):21-5. pmid: 11907475
Rajavi Z, Lashgari A, Sabbaghi H, Behradfar N, Yaseri M. The Incidence of Reoperation and Related Risk Factors Among Patients With Infantile Exotropia. J Pediatr Ophthalmol Strabismus. 2017;54(1):22-30. doi: 10.3928/01913913-20160926-02 pmid: 27783093
Yam JC, Wu PK, Chong GS, Wong US, Chan CW, Ko ST. Long-term ocular alignment after bilateral lateral rectus recession in children with infantile and intermittent exotropia. J AAPOS. 2012;16(3):274-9. doi: 10.1016/j.jaapos.2012.01.005 pmid: 22681946
Parks M. Concomitant esodeviations. In: Tasman W, Jaeger E, editors. Duane's Clinical Ophthalmology. Philadelphila: Lippincott, Williams & Wilkins; 2000. p. 12.
Rajavi Z, Sabbaghi H, Baghini AS, Yaseri M, Moein H, Akbarian S, et al. Prevalence of Amblyopia and Refractive Errors Among Primary School Children. J Ophthalmic Vis Res. 2015;10(4):408-16. doi: 10.4103/2008-322X.176909 pmid: 27051485
Jang GJ, Park MR, Park SC. Bilateral lateral rectus resection in patients with residual esotropia. Korean J Ophthalmol. 2004;18(2):161-7. doi: 10.3341/kjo.2004.18.2.161 pmid: 15635830
Shin DB, Lee YH, Lee SB, Xu YG, Min BM. Effect of Both Lateral Rectus Resection for Residual Esotropia. J Kor Ophthalmol Soc. 2003;44(5):1139-45.
Morrison DG, Emanuel M, Donahue SP. Surgical management of residual or recurrent esotropia following maximal bilateral medial rectus recession. Arch Ophthalmol. 2011;129(2):173-5. doi: 10.1001/archophthalmol.2010.361 pmid: 21320962
Lueder GT, Galli M. Comparison of lateral rectus muscle re-recession and medial rectus muscle resection for treatment of postoperative exotropia. Am J Ophthalmol. 2015;159(4):812-5. doi: 10.1016/j.ajo.2015.01.020 pmid: 25634535
Suh YW, Seo IH, Cho YA, Kim SH. Analysis of the effects of medial rectus muscle resection for recurrent exotropia. Korean J Ophthalmol. 2011;25(5):341-3. doi: 10.3341/kjo.2011.25.5.341 pmid: 21976942
Kim WJ, Kim MM. The clinical course of recurrent intermittent exotropia following one or two surgeries over 24 months postoperatively. Eye (Lond). 2014;28(7):819-24. doi: 10.1038/eye.2014.93 pmid: 24788017
- Abstract Viewed: 1511 times
- Full Text PDF Downloaded: 1125 times
